Multimodal Treatment Of A Difficult CD Wound - Case Report
Jason Swoger, MD, Gastroenterology, 05:52PM Dec 4, 2010
Many of the physicians in our group have been working with a 23 year-old female with a complex recent medical presentation. She was diagnose with Cronhs Disease at the age of 15. Prior therapies had included 5-ASA medications, 6-MP, infliximab, and adalimumab. She had complications of infection/sepsis after initiating adalimumab. She eventually underwent colectomy with a Hartman's pouch, complicated by an intrasphincteric fistulas, involving the Hartman's pouch, and necessitating a completion proctectomy in 12/2009. The proctectomy was complicated by wound dehisence and poor wound healing at the umbilicus, as well as in the perineum. Antibiotics and wound debridements were not helpful. She was being treated with low dose methotrexate, as well as low-dose prednisone for secondary adrenal insufficiency. In June 2010, she began hyberbaric oxygen therapy to attempt to improve wound healing. The umbilical wound healed, but the perineal wound continued to be problematic. It was thought that the wound would partially heal, leading to the accumulation of infected fluid in the perineal cavity. An EUA was performed, and found a deep sinus tract reaching into the sacral hollow. Granulation tissue was present, but there was no evidence of healing. The depth of the wound at this time was approximately 22-25cms, and a picture of an endoscopic examination of the wound is seen below.
Jason Swoger, MD, Gastroenterology, 05:52PM Dec 4, 2010
Many of the physicians in our group have been working with a 23 year-old female with a complex recent medical presentation. She was diagnose with Cronhs Disease at the age of 15. Prior therapies had included 5-ASA medications, 6-MP, infliximab, and adalimumab. She had complications of infection/sepsis after initiating adalimumab. She eventually underwent colectomy with a Hartman's pouch, complicated by an intrasphincteric fistulas, involving the Hartman's pouch, and necessitating a completion proctectomy in 12/2009. The proctectomy was complicated by wound dehisence and poor wound healing at the umbilicus, as well as in the perineum. Antibiotics and wound debridements were not helpful. She was being treated with low dose methotrexate, as well as low-dose prednisone for secondary adrenal insufficiency. In June 2010, she began hyberbaric oxygen therapy to attempt to improve wound healing. The umbilical wound healed, but the perineal wound continued to be problematic. It was thought that the wound would partially heal, leading to the accumulation of infected fluid in the perineal cavity. An EUA was performed, and found a deep sinus tract reaching into the sacral hollow. Granulation tissue was present, but there was no evidence of healing. The depth of the wound at this time was approximately 22-25cms, and a picture of an endoscopic examination of the wound is seen below.
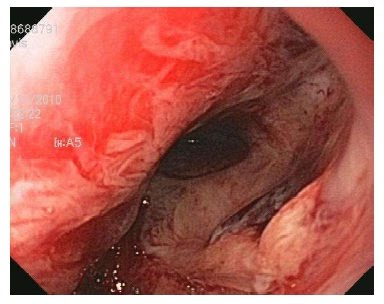
The patient had not tolerated a wound vac in the past, due to significant pain, especially with dressing changes. However, it was thought that there was potential for the wound to heal. The decision was made to have the patient undergo woundvac changes under propofol sedation. In addition, the tissue in the sinus tract was manipulated using different methods, in order to stimulate the formation of granulation tissue and healing. Scraping and abrasion was performed with a gauze covered hemostat, a biopsy brush through the instrument channel of a endoscope, and APC (argon plasm
 a coagulation). The photo below shows progress about 1/2 way through the treatment sessions, which occurred twice a week, and coincided with woundvac changes.
a coagulation). The photo below shows progress about 1/2 way through the treatment sessions, which occurred twice a week, and coincided with woundvac changes.
The wound continued to show improvement, in both size and granulation. At the most recent woundvac changing, the depth of the cavity had improved to only 4-5cm, and a picture of the lining of the sinus tract is below. There has not been much interval change over the past few treatment sessions, and we are considering another trial of hyperbaric oxygen in order to complete the healing process. I though this was an interesting case, using creative and multimodal means to address a very complex and severe Crohn's disease related issue that is not often seen in practice.

No comments:
Post a Comment